 Welcome to the United Nations
Welcome to the United Nations



INTRODUCTION
Converging crises such as the COVID-19 pandemic, the war in Ukraine, climate change and various conflicts, have become a defining challenge of our time. Crises that might have previously been contained within a specific geographic space are now propagated rapidly through globally interconnected systems and networks in areas such as economics, finance, the environment and health.

This Policy Brief highlights the following: (a) converging crises have reversed and exposed the fragility of global SDG progress and imposed high costs on developing countries, (b) reducing inequality and poverty is critical to building resilience against the impact of shocks and crises, and (c) investment in the SDGs, particularly those that underpin social development, can help build resilience of developing countries to multiple crises, as seen in the case of the COVID-19 pandemic.
Converging crises have stalled and even reversed global SDG progress
The world is not on track to achieve the SDGs by 2030. The 2024 assessment of the roughly 140 targets with data shows that only 17 per cent are on track and over one-third have seen either no movement or regressed below the 2015 baseline (United Nations, 2024a).
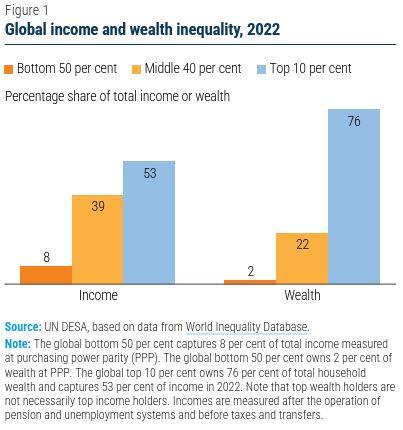
Recent crises have exacerbated global inequality (SDG 10), with the world’s richest people doubling their income during the COVID-19 pandemic, while 99 per cent of humanity became worse off (Independent Group of Scientists appointed by the Secretary-General, 2023). The richest 10 per cent of the global population currently takes an estimated 52 per cent of global income, whereas the poorest half earns 8.5 per cent (figure 1) (Chancel, L., et al., 2022). Wealth concentration is even more pronounced, with the poorest half of the global population owning only 2 per cent of global wealth, while the richest 10 per cent hold 76 per cent. Furthermore, total billionaire wealth increased by $2 trillion in 2024 alone, much faster than in 2023 (Oxfam International, 2025).
Converging crises have materially affected the development prospects of developing countries, which has contributed to a reversal in SDG progress (United Nations, 2024b). This impact has been particularly borne by the most vulnerable groups in society.
THE SOCIAL DETERMINANTS OF SHOCKS AND CRISES
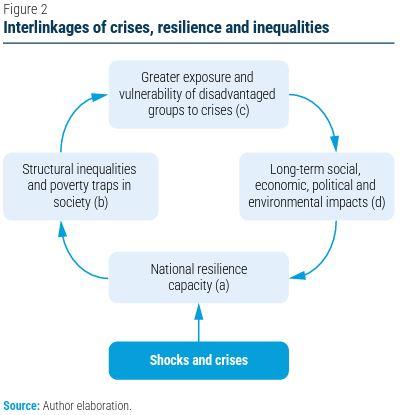
How shocks and crises impact countries depends on their resilience capacity, or the ability to withstand and recover from such adversities (figure 2, step a).
The resilience capacity is determined by factors such as the ability of the economy to create jobs and grow, the state of human development, social cohesion, infrastructure, healthcare system, governance and public administration and trust in institutions, and the way in which countries manage their natural resources—all critical SDG areas.
The role of human development and social cohesion is reflected in the impact of structural inequalities and poverty traps on resilience capacity (figure 2, step b). Structural inequalities exist when a group of people are systematically disadvantaged compared to others based on factors like race, gender, ethnicity, wealth or cultural differences. Poverty traps are created by a combination of lack of material assets and human capabilities.
High inequality and poverty in society increase the exposure and vulnerability of disadvantaged groups to the impact of shocks and crises (figure 2, step c). Research shows that unequal societies are more vulnerable to floods, droughts, pandemics and other natural disasters (United Nations, 2016). Severe poverty and inequality and low levels of human development also limit the capacity of poor households to manage climate and other natural disaster risks, which raises the likelihood of environmental shocks.
COVID-19 revealed alarming inequalities in infection, hospitalization and mortality among populations within and among countries (WHO, 2021). Disadvantaged groups, such as older people, were significantly more affected.
The decreased trust in society that stems from structural inequalities and poverty traps also undermines resilience when faced with a shock or crisis because disparities are likely to weaken the national capacity for collective action that requires citizens to make short-term sacrifices for long-term benefits.
Shocks and crises are likely to have long-term economic, social, political and environmental impact, particularly in developing countries, and materially weaken their resilience capacity (figure 2, step d). Some of these long-term impacts may include population displacement; rising inequality; health crises; recession and unemployment; high debt burden; supply chain disruptions; increased polarization in society; resource depletion; pollution; climate change; and loss of biodiversity.
HOW SDG PROGRESS WAS ASSOCIATED WITH STRONGER RESILIENCE IN THE CASE OF COVID-19
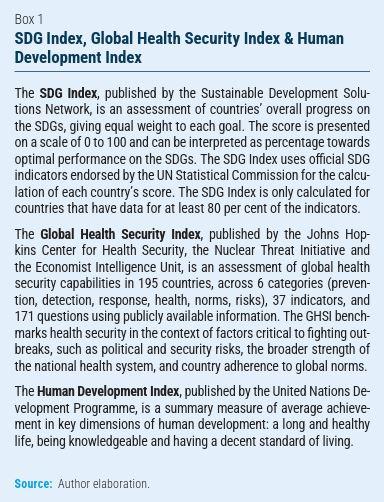
The COVID-19 pandemic resulted in millions of lives lost around the world. However, some developing countries were better able to respond to the crisis and mitigate the health, social and economic costs. Progress on the SDGs, particularly those that underpin social development, emerges as an important explanatory variable for a less severe health impact of COVID-19 in some developing countries. A lower number of lives lost due to COVID-19 is generally correlated in those countries with better scores on indicators that can be used as a proxy for SDG progress, such as the SDG Index, the Global Health Security Index (GHSI) and the Human Development Index (HDI) (box 1).
A robust healthcare system
Experience shows that countries with robust healthcare systems with universal access performed better in dealing with the COVID-19 crisis (Islam, S. N., et al., 2020). A lowincome level was not an insurmountable obstacle to success in dealing with the pandemic.
More than 90 per cent of the Rwandan population had health insurance at the start of COVID-19 in 2020 and the country spent 7.8 per cent of the government budget on health, well above the regional average. The combination of preparedness and prior investments in healthcare, along with determined early measures such as a rapid vaccine rollout, enabled the country to stem the spread of the COVID-19 virus. The Johns Hopkins Coronavirus Resource Center estimates that Rwanda, with a population of 14 million and ranked 173rd on GDP per capita in 2019, had 133 thousand confirmed COVID-19 cases and lost 1,468 lives, with a case-fatality rate of 1.1 per cent, almost equal to the global average of 1 per cent. In 2019, Rwanda ranked 117th on the Global Health Security Index (table 1) but 89th on the sub-indicator assessing the strength of the national health system and 126th on the SDG Index, well above its GDP per capita position.
The Johns Hopkins Coronavirus Resource Center estimates that Bangladesh with a population of 173 million and ranked 149th on GDP per capita in 2019, had 2.3 million confirmed COVID-19 cases and lost 29,000 lives, with a casefatality rate of 1.4 per cent, compared to the global average of 1 per cent. The country was ranked 113th on the Global Health Security Index in 2019 and 95th in 2022 (table 1), including 49th on the sub-indicator assessing the strength and quality of laboratory systems, laboratory supply chain, real-time surveillance and reporting capacities for epidemics of potential international concern. Bangladesh is also one of the countries that have made the greatest progress on the SDGs since 2015 (Sachs, et al., 2024), moving up 12 places on the SDG Index between 2019 and 2022 despite the impact of the pandemic.
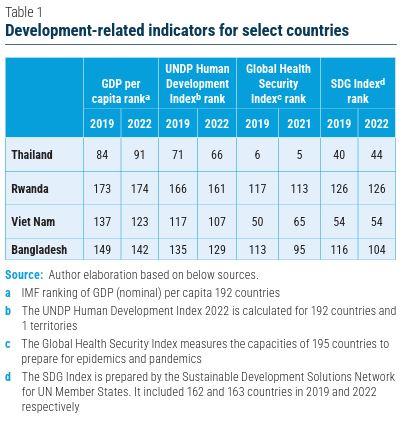
Like Rwanda, Viet Nam was a global leader in the rapid rollout of the COVID-19 vaccine (Hoang, 2022). The Johns Hopkins Coronavirus Resource Center estimates that Viet Nam, with a population of almost 100 million and ranked 137th on GDP per capita in 2019, had 11.6 million confirmed COVID19 cases and lost 43,000 lives, with a case-fatality rate of 0.4 per cent, well below the global average of 1 per cent. The country ranked 50th and 65th on the Global Health Security Index (GHSI) in 2019 and 2021, in both years well above what its GDP per capita would suggest (table 1). The country also ranked 29th on the detection and reporting sub-indicator of the GHSI in 2021; 117th on the Human Development Index in 2019 but had moved up ten places by 2022; and 54th on the SDG Index in both 2019 and 2022.
A universal health coverage scheme in Thailand, initiated in 2002, has rapidly expanded access to healthcare and improved outcomes, particularly for poor and rural populations. The Johns Hopkins Coronavirus Resource Center estimates that Thailand with a population of almost 72 million and ranked 84th on GDP per capita in 2019, had 4.7 million confirmed COVID-19 cases and lost 33,000 lives, with a case-fatality rate of 0.7 per cent, well below the global average of 1 per cent. Thailand ranked 6th and 5th on the Global Health Security Index in 2019 and 2021, well above its GDP per capita position (table 1). In addition, on the sub-indicator of the GHSI assessing the strength of the national health system, the country ranked second in 2019 and on the detection and reporting sub-indicator, it ranked first in 2021.
A shock-responsive social protection system
Research and simulations of eight developing economies show that investment in social protection generates economic growth; creates new jobs; increases tax receipts; reduces poverty; and lowers barriers to women entering or returning to work (ITUC, 2021). An investment of 1 per cent of GDP in social protection can generate a cumulative effect on real GDP ranging from 3.2 to 7.0 per cent over a 10-year period. Such investment appears to have particularly strong impact on countries with low GDP per capita.
South Africa has established one of the most comprehensive social protection systems among developing countries involving social grants, including pensions, disability payments, and child support to provide financial security and support to vulnerable populations, alongside other services such as free basic education and healthcare. The political commitment to social security proved critical in limiting the impact of COVID-19 on poverty and inequality, as the pandemic was one of the largest shocks in the country’s history. GDP in the second quarter of 2020 was 17 per cent lower than in the second quarter of 2019 (IFPRI, 2021). However, a large-scale programme of tax-financed social protection was key to building resilience against this very high decline in economic output, with the GDP falling by 6 per cent and 4 per cent in the third and fourth quarters respectively compared to the same quarters in 2019. The large public investment in social protection in the early stages of COVID-19, where the government reached more than 30 million people, proved critical in stabilizing demand in the economy and lowering the impact of the pandemic on both individuals and communities and this intervention is considered the most effective of its kind on the continent (Gronbach, et al., 2022).
Uruguay stands out in Latin America for its low level of inequality and poverty. Uruguay accords high priority to SDG implementation and was ranked 34th on the SDG Index in 2024 (Sachs, et al., 2024) and 52nd on the Human Development Index in 2022 (UNDP, 2024). Uruguay’s social policy response to COVID-19 greatly benefited from its long history of investment in this area, which allowed the country to rapidly expand social, economic and financial measures.
Uruguay stood out in the region for avoiding the worst of the COVID-19 pandemic, with no exponential growth in infections and a low death toll, unlike many of its neighbouring countries. The low level of poverty and inequality, as well as the country’s compliance with international health regulations, played an important role in enabling Uruguay to effectively mitigate the health costs of COVID-19. Uruguay’s GDP per capita declined by 6 per cent in 2020, but without the social, economic and financial mitigation measures adopted at the outset of COVID-19, the output contraction would have been much larger and the recovery in 2021 and 2022 not as robust (Bucacos, et al., 2023). By 2023, the unemployment rate in Uruguay was 7.8 per cent, lower than the 8.5 per cent in 2019, prior to the COVID-19 pandemic.
CONCLUSION
Converging crises have become a defining challenge of our time. They have imposed high economic and social costs on developing countries and stalled, and in some cases reversed, global progress on the SDGs.
The COVID-19 experience shows that developing countries that had invested in the achievement of the SDGs, particularly those that underpin social development, were better able to deal with the impact of the pandemic.
Historically, crises have often acted as a catalyst for social policy reform. This was the case with the “New Deal” in the United States during the Great Depression in the 1930s; the 1945 welfare reform in the United Kingdom; the expansion of welfare states in European countries after World War II; and the social policy reform in East Asia following the 1997 financial crises. Crises galvanize social movements that push for measures to address systemic weaknesses such as inequality and poverty.
The way forward
1. Reducing inequality and poverty and strengthening healthcare and social protection is critical to building resilience against the impact of shocks and crises.
2. Strengthening health systems in developing countries should not be seen as a task of those countries alone but of the international community as a whole.
3. Ensuring universal social protection is critical for enhanced resilience of vulnerable populations, the economy and political and social stability.
4. The Second World Summit for Social Development in 2025 provides an opportunity to reinvigorate the SDG momentum and build a new consensus among all stakeholders on complementary national and global action for advancing social development.