 Welcome to the United Nations
Welcome to the United Nations


INTRODUCTION

In 1994, the International Conference on Population and Development (ICPD), held in Cairo, ushered in a paradigm shift that would reshape how governments formulate and implement population policies. While recognizing the advantages of population stabilization for sustainable development, the ICPD Programme of Action, adopted by 179 United Nations Member States, affirmed that national policies pertaining to population and development must have at their core a fundamental respect for human rights. The following year in 1995, at the Fourth World Conference on Women in Beijing, 189 countries adopted the Beijing Declaration and Platform for Action. Within their broad scopes, the Cairo Programme of Action and the Beijing Platform for Action emphasized the importance of family planning for fulfilling the basic right of individuals and couples to decide the number, spacing and timing of their children and to have the information and means to do so, and the right to achieve the highest attainable standard of sexual and reproductive health. The two documents highlighted that ensuring universal access to sexual and reproductive healthcare services, including for family planning, information and education, is critical for protecting the rights and futures of girls and women.
The follow-up to the Beijing and Cairo conferences provided a basis for including and monitoring objective targets on family planning and reproductive health within international frameworks, including the Millennium Development Goals (MDG 5) in 2005 and the Sustainable Development Goals (SDGs 3 and 5) in 2015. The centrality of reproductive health to women’s empowerment is also reflected in the inclusion of indicators on the adolescent birth rate (SDG indicator 3.7.2) and modern contraceptive use (SDG indicator 3.7.1) in the Women’s Empowerment Index (WEI), which measures women’s power and freedom to make choices and seize opportunities in life (UN Women and UNDP, 2023).
Within the broad picture of progress and stalls in sexual and reproductive health (see box 1), this policy brief will examine in more depth the changes in adolescent birth rates and family planning in the context of global fertility decline over the last 30 years. It will highlight inequalities in those changes and discuss the challenges of living up to the commitments made at Cairo and Beijing moving forward.
THE CHANGING DEMOGRAPHIC CONTEXT: TOWARDS LOW FERTILITY
In 2024, the global fertility rate stood at 2.2 births per woman on average, down from 2.9 in 1994. Even in countries with relatively high fertility levels, the average number of births per woman has declined. While more than 1 in 10 countries and areas (13 per cent)—mostly in sub-Saharan Africa, but also Afghanistan, Sudan and Yemen—still have fertility levels of 4 or higher, this represents a decline from around one third of countries and areas in 1994 (United Nations, 2025).

Low fertility is common today, with more than half of all countries and areas (55 per cent) having fertility levels below 2.1 births per woman. This group crosses all regions and income categories and contains more than two thirds of the global population. By comparison, in 1994, less than a third of countries and areas (31 per cent) had fertility levels below the threshold of 2.1. Today, in more than a tenth of countries and areas globally, fertility is below 1.4 births per woman. In four countries—China, the Republic of Korea, Singapore and Ukraine—it is below 1.0. If sustained over decades, fertility levels below 1.4 births per woman result in rapid population decline and a pronounced shift in the population age distribution towards older ages. In this changing demographic context, some governments have become concerned about low fertility and have adopted policies aimed at increasing the birth rate. Even in the face of these demographic changes, it is critical that access to sexual and reproductive healthcare and fulfilment of reproductive rights remain imperatives and that associated policies embody a fundamental respect for human rights.
ADOLESCENT CHILDBEARING HAS DECLINED, BUT GIRLS IN SOME REGIONS ARE STILL AT HEIGHTENED RISK
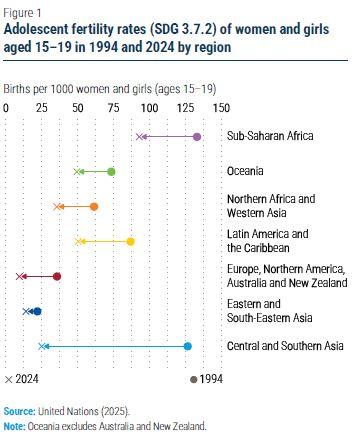
Adolescent girls have become substantially less likely to give birth (figure 1). In every region of the world, the adolescent fertility rate (SDG indicator 3.7.2) in 2024 had decreased by at least 30 per cent compared to 1994; it had decreased by more than 80 per cent in Central and Southern Asia. The ubiquitous decline of the adolescent birth rate has been one of the major success stories in population health over the past three decades, allowing more young women and girls to complete their schooling and avoid health complications from early pregnancies. Nevertheless, much work remains to be done. In sub-Saharan Africa, nearly 1 in 10 young women and girls aged 15–19 years give birth each year, a rate that is far higher than in other parts of the world. Of 4.7 million babies born annually to mothers below age 18 worldwide, more than half are born in sub-Saharan Africa; of 340,000 babies born to girls below age 15, nearly 70 per cent are born in sub-Saharan Africa (United Nations, 2025).
While child marriage continues to be a major pathway to early childbearing, the situation today is diverse across countries with high adolescent birth rates. In several countries, first births to girls below age 18 occur more frequently outside of marriage than within (Molitoris and others, 2023). In this context, the failure to meet adolescent needs for family planning is an important contributor to early childbearing. Sexually active adolescent girls who want to avoid pregnancy are far less likely to use a modern contraceptive method than women at older ages (United Nations, 2022). Academic research and programmatic experience have shown that the most successful interventions for meeting adolescent contraceptive needs and reducing adolescent childbearing are those that focus on the needs of adolescents and young women by offering school-based sexuality education, providing adolescent-responsive care, overcoming biases and misconceptions among health service providers and implementing laws and policies that support access to contraception regardless of age or marital status (Chandra-Mouli and Akwara, 2020).
Addressing the factors that lead to child marriage and early childbearing, including economic hardship, lack of economic opportunities for women and strong social norms supporting the practice, has proven effective in reducing the number of child marriages and births to adolescents (Psaki and others, 2021). Such interventions may also help alleviate pressures from social norms that support child marriage and early childbearing, which are often reinforced by poor economic conditions. It is also crucial that countries not only implement but also enforce laws forbidding child marriage.
MORE WOMEN THAN EVER ARE USING MODERN CONTRACEPTIVE METHODS
Concurrent with the fertility decline and postponement of childbearing during the past 30 years, more women want to avoid pregnancy over longer periods of their reproductive lives. Globally, the number of users of modern contraceptive methods has increased by 58 per cent over the past 30 years, rising from 552 to 871 million between 1994 and 2024. In 1994, about 70 per cent of women aged 15–49 years who wanted to avoid pregnancy used a modern method to do so (SDG 3.7.1); today, nearly 78 per cent use modern methods. Despite this progress, there are still more than 250 million women of reproductive age who want to avoid pregnancy but are not using modern contraception (United Nations, 2024).
There have been substantial changes at the regional level over the past 30 years (figure 2). In sub-Saharan Africa, the percentage of women wanting to avoid pregnancy who used a modern method of contraception nearly doubled, from 29 per cent in 1994 to 57 per cent in 2024. While progress has been remarkable, levels of contraceptive use in the region are still significantly below the global average. There are many reasons for these discrepancies, including: limited knowledge about contraception and fecundity; lack of or limited access to modern contraception; social and religious norms that make some women less likely to seek information, services and commodities; and lack of reproductive autonomy within relationships, especially in contexts of child or early marriage. Improved access to sexual and reproductive healthcare and education, especially among economically vulnerable and marginalized women and those living in remote areas, would help to address the challenges associated with early childbearing and unintended pregnancies.

Contraceptive methods vary widely in their effectiveness at preventing pregnancy, their ease of use, their potential side effects and their popularity. Modern contraceptive methods (e.g., intra-uterine devices (IUDs), hormonal pills, implants and injectables) are generally far more effective at preventing pregnancy than traditional methods (e.g., rhythm methods and withdrawal). Nevertheless, preferences and actual use of specific methods vary across countries owing to a combination of factors, including method availability and accessibility, compatibility of specific methods with religious or cultural norms, changes in fertility intentions, and systematic external influences (e.g., family planning programs and government initiatives).
Among women aged 15–49 years, the distribution of contraceptive users by method differs substantially across regions (figure 3). Whereas at the population level, the use of contraceptive methods changes only gradually (United Nations, 2022), individual preferences for specific methods are dynamic, and users often change their preferences for specific methods in response to changes in life circumstances. It is important that women and couples have access to a full range of safe, effective and affordable contraceptives, along with the information and education necessary to utilize them effectively.

NATIONAL AND INTERNATIONAL COMMITMENTS TO REPRODUCTIVE HEALTH MUST BE SCALED UP
Countries should accelerate progress towards universal healthcare coverage to deliver essential healthcare services in an inclusive, equitable, cost-effective and efficient manner while protecting, respecting and fulfilling the human rights of all persons, including their reproductive rights, and recognizing the additional investments and renewed political commitment needed. Comprehensive sexual and reproductive healthcare services are essential for ensuring healthy lives and well-being for all at all ages, and the necessary investments per capita are modest and affordable for most countries (Starrs and others, 2018). Less developed countries face funding gaps that will likely be overcome only through a combination of domestic and international financing. Yet, recent trends have shown that sufficient international financing is far from guaranteed. National and international investments in reproductive health care services must be scaled up, particularly in countries with rapidly growing numbers of women of reproductive age. For example, in the least developed countries, the number of women aged 15–49 will increase by 13 per cent between 2025 and 2030 and by 65 per cent between 2025 and 2050.
Countries must also take actions beyond the health sector to promote gender equality. Discrimination and legal barriers often restrict women’s and adolescents’ autonomy in making decisions about their sexual and reproductive health. Investing in programmes to end child marriage, empowering women in reproductive decision-making and integrating family planning and reproductive health into primary healthcare can raise women’s level of education, facilitate their economic participation and reduce rates of unintended pregnancy and early childbearing.